
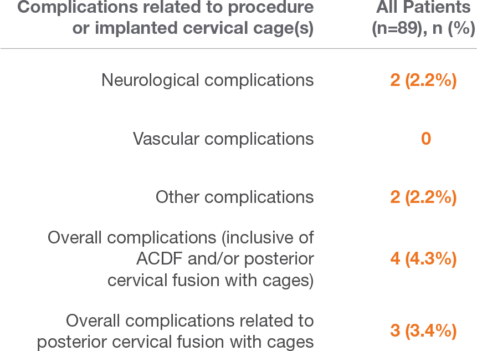
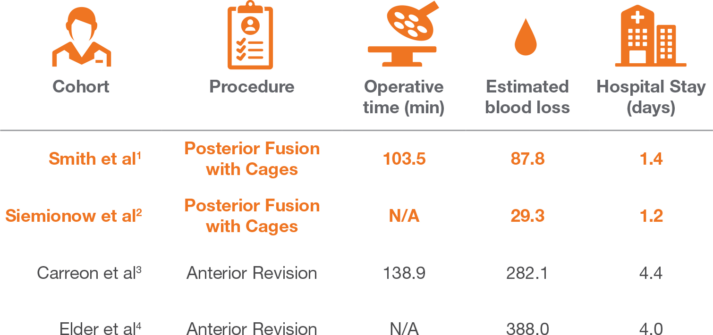
Posterior Fusion vs. Anterior Revision For Symptomatic Pseudarthrosis
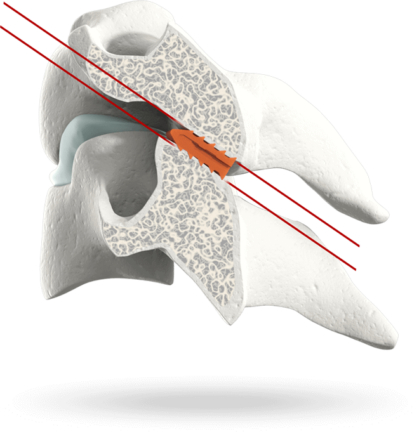
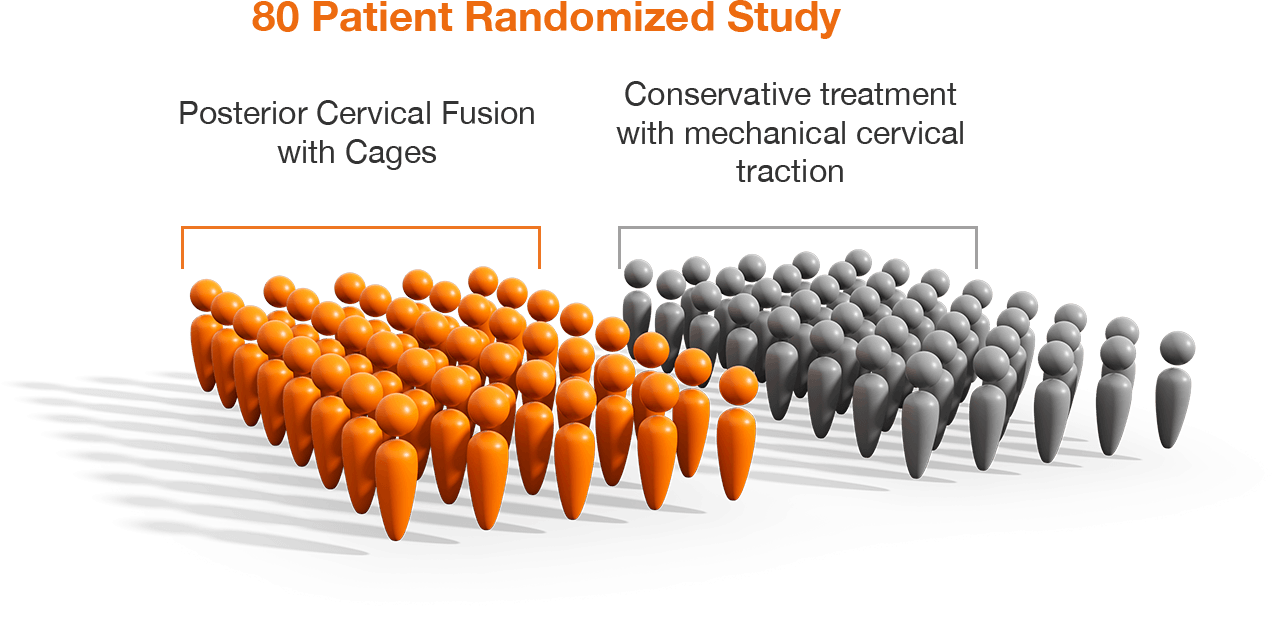
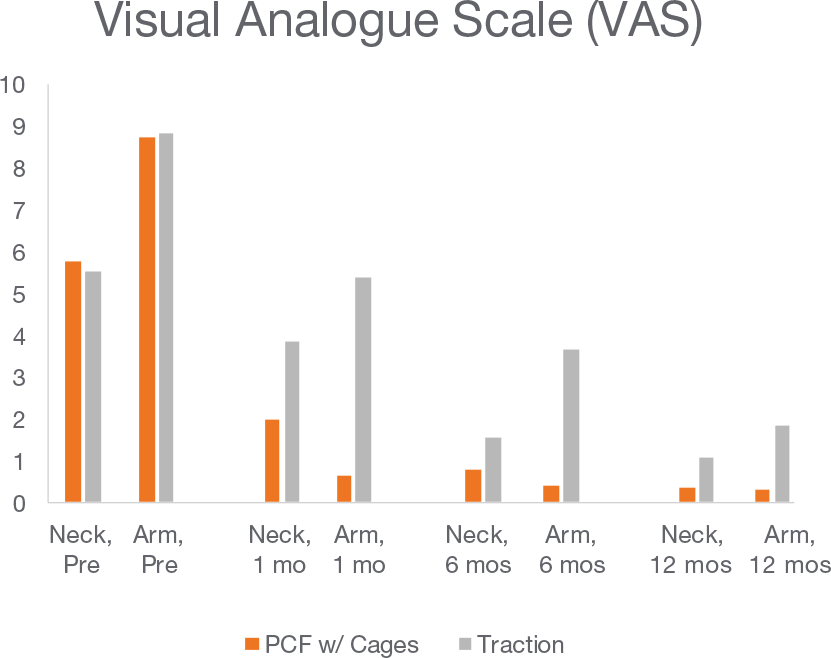
PCF with Cages vs. Traction Single Level Cervical Radiculopathy 80 Patients @ 1-year follow-up
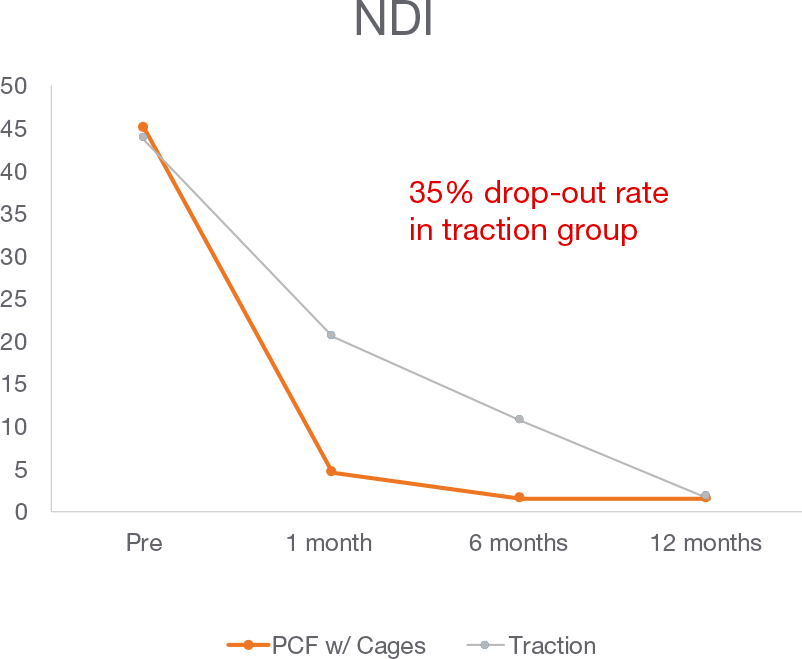
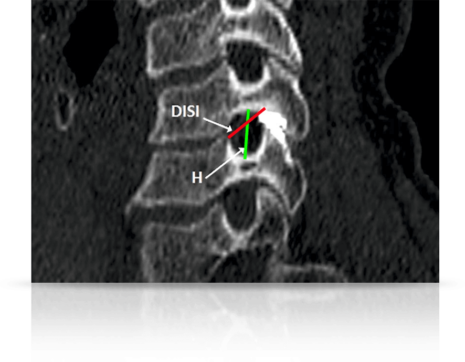

Posterior Cervical Fusion with Cages does not significantly change cervical alignment.